Coronavirus: why we’re investigating the long-term impact on hearing

While the pace of research on the novel coronavirus has been impressively rapid, there remains a lot we still don’t know about the wily pathogen. One of those unknowns is the potential long-term health implications for people who have had the disease.
There has been an avalanche of research on the virus, but the immediate priority has been to report on epidemiology, diagnosis, treatment, vaccines and antibody tests. However, there is already growing evidence that COVID-19 is not a simple lung infection. Why, for example, is asthma when it is a major risk factor for influenza?
There may well be long-term health consequences for a variety of organ systems that extend beyond the respiratory system, including the , and . And there may be implications for health disciplines that are seemingly unrelated to COVID-19. For example, there are reports of headaches, blood clots, digestive problems and the .
It is well known that viruses such as . And coronaviruses can cause peripheral neuropathy, damage to the nerves that . It is possible, in theory, that COVID-19 could cause auditory neuropathy, a hearing disorder where the cochlea is functioning but transmission along the auditory nerve to the brain is impaired. People with auditory neuropathy have difficulty hearing when there is background noise, such as in a pub.
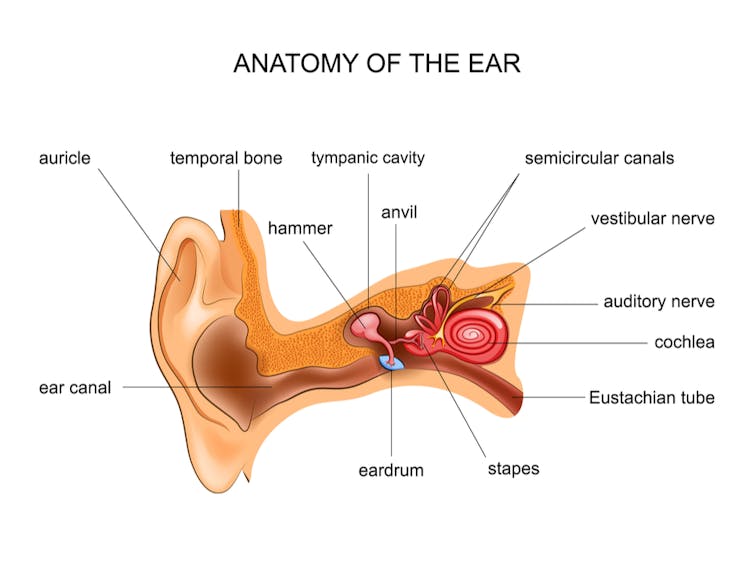 Anatomy of the ear, showing the cochlear and the auditory nerve that carries the sound signal to the brain.
Anatomy of the ear, showing the cochlear and the auditory nerve that carries the sound signal to the brain.
Auditory neuropathy has been linked with Guillain-Barré syndrome, an acute immune disease that affects central and peripheral nerves. Importantly, COVID-19 is also .
Low-quality evidence, but we need to be ready
There are unsubstantiated and anecdotal cases of COVID-19 and hearing loss reported in . But my colleagues and I wanted to know if there was any more robust evidence this, so we conducted a systematic review of the available evidence. Our review, , found reports of hearing loss and tinnitus, but there were only a small number of studies and the quality of evidence was low.
It is important not to diagnose hearing loss where it does not exist, or where it is coincidental given the high rates of COVID-19 in the population. On the other hand, the findings of our review might simply reflect the start of our understanding of this emergent health condition. We need to be prepared to act.
A physician friend of mine working in 91ֱ�� told me they have surveyed COVID-19 patients after discharge from hospital and, so far, three out of 25 have reported problems with their hearing. Until the data have been published in a peer-reviewed journal we need to treat it cautiously, but it does provide a possible early indication of what might be to come.
Because of the need to provide timely evidence for decision-makers on this urgent and emergent health issue, we are planning to repeat our review of COVID-19 and hearing loss at regular intervals over the coming year. It is likely that other health disciplines will follow suit. Health conditions may emerge over time that have clear clinical relevance. Following up with COVID-19 patients will probably teach us a lot about the long-term consequences of this destructive disease.![]()
, Ewing Professor of Audiology,
This article is republished from under a Creative Commons license. Read the .